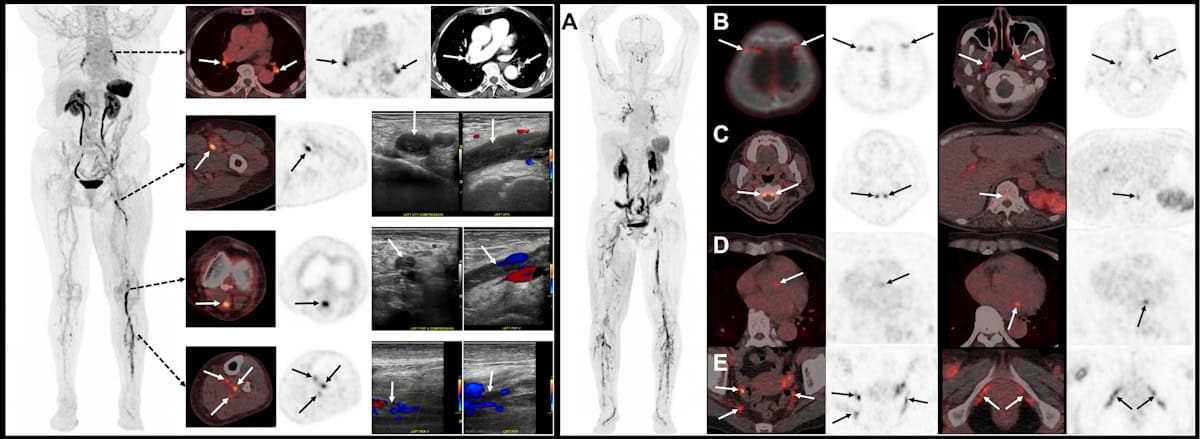
Image of the year Left: 18F-GP1 PET/CT images showing multiple blood clots in the deep veins of the left leg, plus several clots in the right calf and clots in both lungs. Right: 18F-GP1 PET/CT images showing widespread blood clots throughout the body. (Courtesy: S Han et al. Asan Medical Center, Seoul, Korea)
A PET radiotracer that can detect deep vein thrombosis (DVT) in the legs and clots that have travelled to the lungs has been chosen as the “Image of the Year” at the Society of Nuclear Medicine and Molecular Imaging (SNMMI) 2026 annual meeting. Developed by Sangwon Han and colleagues at the Asan Medical Center, University of Ulsan College of Medicine, in Korea, the novel tracer enables whole‑body imaging of blood clots (thrombi) in the legs and lungs in a single scan.
A DVT is a blood clot that forms in a deep vein, usually in the legs. It’s a common condition, with an incidence of roughly half that of all cancers, and it can lead to serious complications. Clots can break off and travel to the lungs, which could cause a potentially life‑threatening pulmonary embolism (a blockage in the artery supplying blood to the lungs). Early detection of DVT is therefore critical for determining the most appropriate treatment for each patient.
Currently, the standard imaging method for diagnosing DVT is venous ultrasonography (VUS). But while this works well for detecting clots in the thigh-to-knee region, whole-leg VUS requires skilled operators and advanced machines, takes longer, and has lower diagnostic sensitivity in the calf. In addition, conventional imaging techniques such as VUS and CT rely on indirect structural changes rather than directly visualizing the clot.
Aiming to enable faster and more efficient DVT diagnosis, Han and his research team are studying fluorinated GP1 (18F-GP1) a novel thrombus-targeted PET tracer. The tracer selectively binds to specific receptors on activated platelets (the cell fragments that cause blood to clots), allowing direct visualization of active thrombus formation.
“In our Phase 1 study, 18F-GP1 PET/CT showed 100% detection rate in 20 patients with confirmed DVT or pulmonary embolism,” Han told the SNMMI delegates. “But that study was limited by its small sample size and an absence of negative groups so specificity could not be assessed at that time.”
So in this latest work, Han and his team performed a phase 2, non-randomized study investigating the ability of 18F-GP1 PET/CT to identify acute lower-extremity DVT in 46 symptomatic patients. This included 22 patients with proximal DVT and 24 with none or distal DVT, as diagnosed using VUS.
The researchers acquired chest-to-feet PET/CT scans approximately 2 h after intravenous administration of 250 MBq of the radiotracer. The images were assessed by three blinded nuclear medicine physicians from different institutions, who assigned focal 18F-GP1 uptake higher than background activity as positive for thrombosis. They classified proximal DVT as clots involving the iliac (pelvic), femoral (thigh) and popliteal veins (behind the knee), and distal DVT as clots confined to the calf veins.
“Our primary objective was to assess the sensitivity and specificity of qualitive 18F-GP1 PET/CT interpretation for proximal DVT,” Han explained. “Secondary objectives included assessing the agreement between PET/CT and VUS for distal DVT, inter-reader reproducibility, exploring the detection of pulmonary embolism and assessing safety.”
When evaluated against VUS as a reference standard, 18F-GP1 PET/CT exhibited high diagnostic accuracy for detecting clots, demonstrating a sensitivity of 95% and a specificity of 92% for proximal DVT. “For distal DVT, both positive and negative agreement between PET/CT and VUS were strong,” added Han. “Inter-reader agreement was also excellent.”
The scans also identified concomitant pulmonary emboli in some patients, as confirmed by CT pulmonary angiography, illustrating the advantage of simultaneously assessing DVT and pulmonary embolism in a single scan. The researchers noted that the radiotracer was well tolerated, with no drug-related adverse events observed.
Speaking in the plenary session when his award was announced, Han shared a “striking image” recorded using 18F-GP1 PET/CT, which showed extensive blood clots, not only in the leg and lungs, but also in many unusual sites, including cranial and spinal vessels, cardiac valves, and vessels in the pelvic region. “This image clearly shows the remarkability ability of fluorinated GP1 to visualize thrombi throughout the body,” he explained.
“We believe this represents an important step towards thrombus-specific imaging,” Han concluded. “The potential of GP1 PET can expand beyond DVTs to many other thrombotic diseases such as embolic stroke or other cardiovascular diseases.”
The SNMMI Image of the Year is the society’s highest award, and the most anticipated, given out in recognition of an image that’s truly cutting-edge and representative of the future of nuclear medicine. This year’s winning image was chosen from nearly 1500 abstracts submitted for the meeting.
“It is truly a great honour to receive the Image of the Year award,” said Han.
Two years ago, the ESTRO 2024 meeting in Glasgow dedicated a conference session to the discussion of upright radiotherapy. In particular, the speakers pondered whether this emerging technique – in which patients are treated sitting up rather than lying down – offers hope of increasing access to advanced radiotherapy, or whether it’s merely hype.
Things have moved on since then. Leo Cancer Care introduced its upright photon therapy system, Grace, and received commercial approval in the US and (just last week) Europe for its Marie upright positioning and CT system. Stanford Medicine recently unveiled the world’s first ultracompact proton therapy facility, pairing Mevion Medical Systems’ compact S250-FIT proton therapy system with the Marie platform. Meanwhile, the body of published research on the feasibility and patient experience of upright treatments continues to grow.
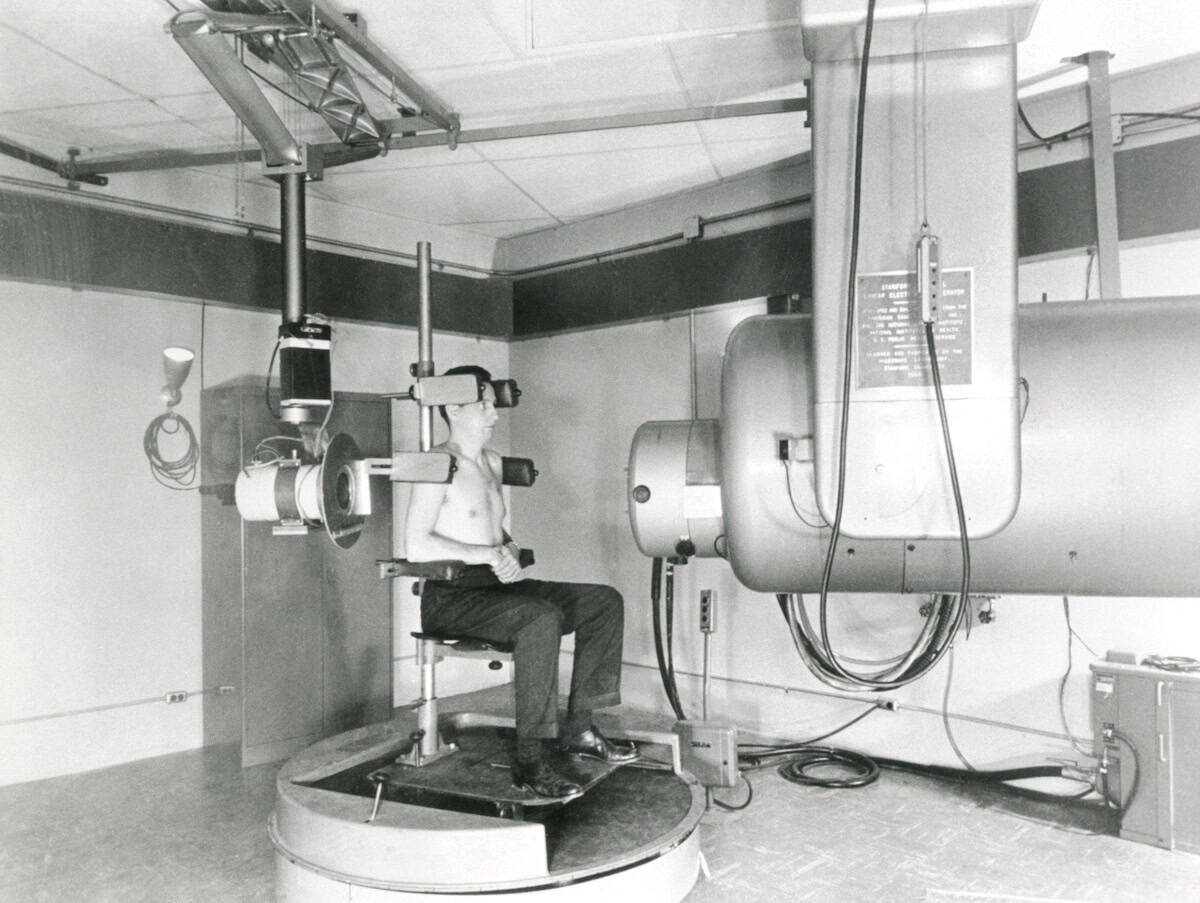
At this year’s ESTRO 2026 meeting in Stockholm, the theme was revisited by four experts in the field, who debated the motion that “Upright radiotherapy will be a mainstream and standard radiotherapy delivery option in 2035”.
The customary pre-debate vote revealed that just one quarter of the audience thought that photon-based upright radiotherapy would become mainstream, with the remainder believing that it would remain a niche technique. When it came to upright proton therapy, however, the vote was split roughly 50:50. So could the speakers persuade the attendees to change their minds?
Patient-centred care
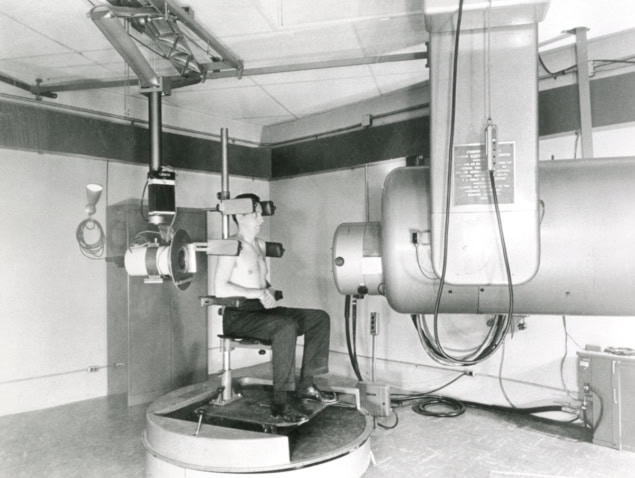
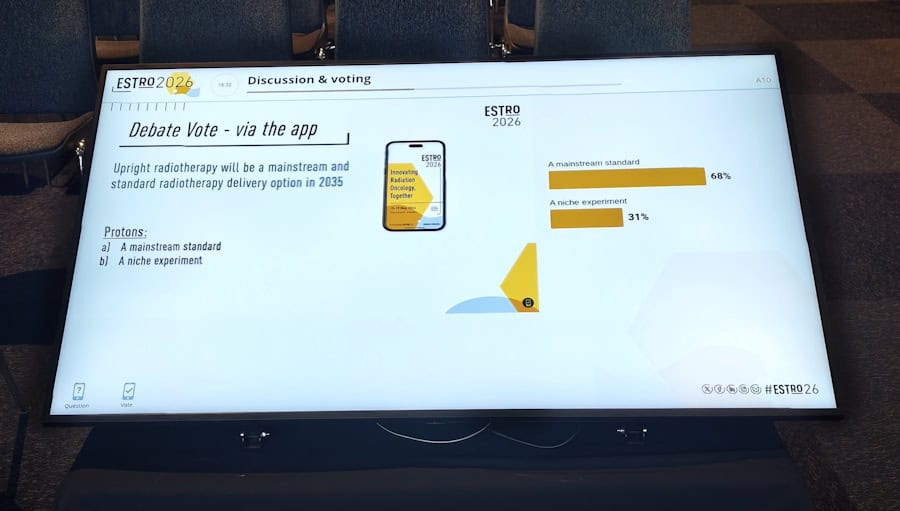
The debate began with Tomas Kron from the Peter MacCallum Cancer Centre in Australia arguing the case for upright X-ray radiotherapy. He pointed out that upright positioning is not a new idea. “Historically, photons and upright have been around for a very long time. It has been, if not standard practice, widely used. But what role will it play in 2035?”
Not a new idea The first high-energy linear accelerator for medical use, known as LA-1, was developed at Stanford in the 1950s. Patients with head-and-neck or lung cancer could sit on an isocentrically mounted chair for treatment. The machine was decommissioned in 1972 and now resides in the Smithsonian Institution. (Courtesy: Stanford Medicine)
Kron described a clinical imaging trial underway at Peter Mac investigating upright cone-beam CT for planning lung cancer radiotherapy. The study showed that image quality was good enough for adaptive treatment planning, and that the lung was expanded and moved less in the upright position. Kron noted that patient setup and imaging was “really, really easy”, taking just a few minutes.
But what’s more important, he emphasized, is the patient experience. Patients treated while sitting up can maintain eye contact with the doctors throughout, they feel more involved and empowered, with one patient commenting: “My breathing was strong, I felt comfortable, the band around my chest was giving me a bear hug.”
“It’s really all about patient-centred care. Physical comfort and emotional wellbeing are top priorities,” Kron said. “Clearly, in an upright scenario this is much more likely to be the case.”
Upright radiotherapy offers many other unique features, including anatomical advantages and the ability to customize the chair, for example, for bariatric or paediatric patients. An upright treatment system is also more compact than a couch-based machine, requiring a smaller bunker. It could also be used as a mobile radiotherapy unit, said Kron – reducing the need for patient travel.
Kron’s team found that 80–90% of their patients could be treated just as well with upright radiotherapy as supine (lying down). “There are anatomical advantages with upright, there are patient preferences, there are economic benefits. What’s not to like,” he concluded.
The myth of mainstream
“Upright radiotherapy will not be mainstream and standard,” declared the second speaker, Livia Marrazzo from the University of Florence in Italy.
“Mainstream means widely adopted, used across the majority of radiotherapy centres, the default in clinical practice … and standard is even stronger, backed by clinical evidence, guideline-endorsed, reproducible and validated,” Marrazzo told the delegates. “It’s not ‘it works in some centres, is technically feasible, has early adopters, may have advantages for some patients’. But that is where we are with upright radiotherapy.”
The art of persuasion Livia Marrazzo argued that upright radiotherapy will not be mainstream by 2035. (Courtesy: Icro Meattini)
From a practical standpoint, most of the roughly 16,000 radiotherapy systems worldwide are linac-based recumbent machines with a typical lifecycle of 10 to15 years. Many were recently replaced with supine systems optimized for intensity-modulated and image-guided radiotherapy. “The installed base is locked into supine geometry for another full cycle,” Marrazzo explained.
She refuted many of the advantages proposed by Kron. “We have limited clinical evidence supporting comfort advantages,” she said. “It may benefit specific patient groups and conditions, but this doesn’t mean mainstream.” Overall, clinical experience is limited, with no comprehensive evaluations of plan quality and no comparative clinical studies.
She highlighted the particular challenges of breast cancer treatments, which account for 25-30% of cases in her radiotherapy department. “When we place a breast cancer patient upright, we lose the natural breast separation, so have much more difficulty in hitting the target and avoiding the contralateral breast,” she explained. “This exemplifies how upright is not a plug-and-play replacement for a conventional supine workflow.”
“Are we sure we would like to have upright as the standard radiotherapy delivery option by 2035 or do we want to push our efforts somewhere else?” Marrazzo concluded. She would prefer a focus on introducing technologies such as AI-driven planning and contouring, fully adaptive workflows, ultra-hypofractionation or biology-guided treatment adaptation. “These are all solutions that can be software-driven, scalable and compatible with existing supine infrastructure.”
The motion for protons
With half of the audience already agreeing that upright proton therapy will become mainstream, Petra Trnkova from Czech Technical University had perhaps a slightly easier task as she presented the case for upright protons. Nevertheless, she began by suggesting that her opponents are simply “scared of progress and won’t accept that, even without evidence, we can move forward in radiotherapy”.
Trnkova reiterated the benefits of upright radiotherapy cited by Kron: favourable patient anatomy, lower installation cost, improved sustainability, and patient-centric management. “For proton therapy, these improvements are much more significant,” she noted.
For starters, upright systems could help address the massive disparity in access to proton therapy around the globe. Sharing a map showing how proton therapy facilities are mostly distributed in wealthy countries, Trnkova noted: “My opponents may tell you that it’s not possible to do this by 2035, but when you look at this map, I ask you, can we wait any longer?”
Saving space The compact S250-FIT proton therapy system is small enough to fit in a standard linac vault. (Courtesy: Stanford Medicine)
Increasing access to proton facilities is enabled by the extreme size reduction when eliminating the need for a large rotating gantry, enabling proton therapy systems small enough to fit in a standard linac vault. Upright proton therapy can also reduce machine complexity, increase rotation speed and lower energy consumption – reducing costs, improving system upgradeability and increasing environmental sustainability.
“Another consequence of smaller facilities is we can really have patient-centred care,” Trnkova added. Recalling the 10 to 15 year linac lifetime mentioned by Marrazzo, she suggested another option: “You can replace your linac with proton therapy. Then you can have the full set of treatments available for each patient”.
Upright proton therapy could also ease the introduction of new treatment techniques, such as proton arc therapy, which offers dosimetric benefits over intensity-modulated proton therapy, but it is difficult to deliver with a gantry. It could also enable in vivo dosimetry, using shoot-through protons for range verification, or mixed-beam delivery of protons and photons.
“Upright positioning offers many opportunities, it’s the only way towards the democratization of proton therapy,” Trnkova concluded. “Stop asking what opportunities upright radiotherapy brings, start asking what you can do to bring it faster to clinical practice.”
The reality check
The final speaker, Carles Gomà from Clinic Barcelona in Spain, reflected upon what makes a good radiotherapy system. “In my view, it’s a three-legged stool: beam delivery, imaging and immobilization,” he said. “And progress comes with a combination of the three.”
For example, focusing too heavily on beam delivery and imaging can lead to immobilization being forgotten. “Immobilization means comfort, and if we are comfortable, we are still,” Gomà explained. “I cannot care less how many papers say patients are more comfortable in an upright position,” he added, pointing out that people will pay five times more to fly in business class where they can lie down.
The other reason cited for moving to upright proton therapy is its lower cost. “But is proton therapy expensive?” Gomà asked. He described the situation in Catalonia, which has a population of eight million and in 2018 spent Euro 42.2M on external-beam radiotherapy. “This is exactly the same cost as one immunotherapy drug for the same population,” he pointed out. “Proton therapy is not expensive; photon therapy is ridiculously cheap.”
Gomà also considered whether “suboptimal protons” are better than photons. “I’m going to answer no,” he said, describing two recent phase III, randomized trials comparing photons with protons for oropharyngeal cancer. The US trial concluded that proton therapy provides a new standard-of-care option, but the UK trial reported no difference between the two modalities.
“Let’s learn from history and not repeat the same mistakes,” he concluded. “True progress is improvement without compromise. If we want to make the stool higher, we have to work on all three legs at the same time.”
The final vote At the end of the debate, the ESTRO delegates strongly supported upright proton therapy. (Courtesy: Ye Zhang)
The debate concluded with decisive a final vote: while support for upright photon therapy reduced a little, over two-thirds of the audience believed that upright proton therapy will indeed become mainstream and standard by 2035.
Writing on LinkedIn, session co-chair Ye Zhang from the Paul Scherrer Institut noted: “The debate sparked an inspiring shift in perspective, with final voting showing slightly increased scepticism toward mainstream upright photon therapy (dropping from 23% to 18% support), but a dramatic surge in favour of upright proton therapy, which jumped from 47% to a 69% majority.”
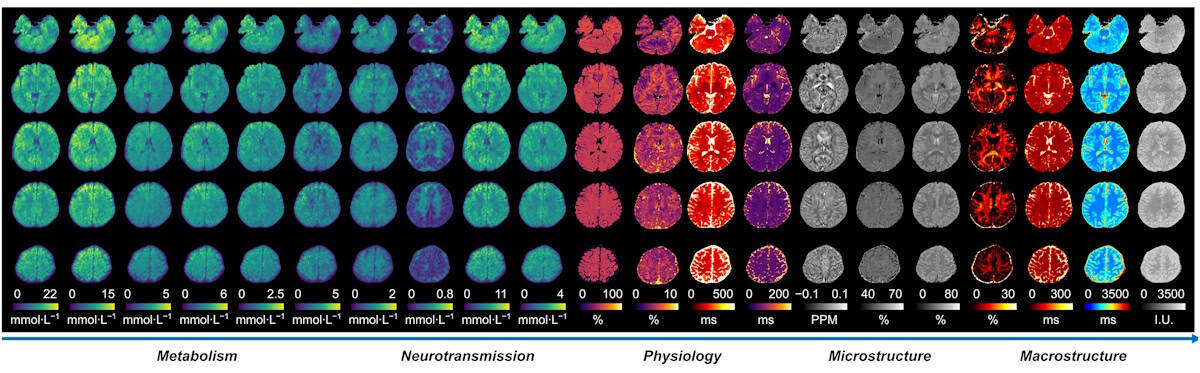
Whole-brain images Biomarkers recorded from a healthy volunteer in a single MRx scan. The information provides a comprehensive spectrum of information on tissue metabolism, neurotransmission, physiological function and structural characteristics. (Courtesy: Yudu Li, University of Illinois)
MRI is a powerful diagnostic imaging tool, with more than 100 million scans performed worldwide each year. While MR signals contain rich information from multiple molecules and numerous physical and biological processes, current clinical MRI exams rely solely on signals from water molecules in tissues and generally only obtain one tissue biomarker at a time. But MRI could do so much more.
A research team headed up at the University of Illinois Urbana-Champaign has done just that, devising a new MRI technique – multiplexed MRI (MRx) – that enables simultaneous mapping of multiple molecular signals using a standard clinical 3 T MRI scanner.
The barrier to performing multiparametric imaging with conventional MRI lies in the “curse of dimensionality”, in which high-dimensional imaging requires prohibitively long scan times. Multimolecular MRI, meanwhile, is limited by weak signals from brain metabolites and neurotransmitters (typically 1000–10,000 times weaker than proton-based signals from water molecules), which often overlap, making them difficult to detect and separate.
“MRx overcomes these challenges through specialized data acquisition and processing strategies,” explains study leader Zhi-Pei Liang. “During data acquisition, MRx simultaneously excites and encodes all detectable molecular signals with sparse sampling to achieve high imaging speed. During data processing, MRx employs physics-driven machine learning methods to separate and quantify the different signal components.”
Reporting their findings in Nature, the researchers demonstrate high-resolution mapping of 22 quantitative biomarkers of the whole brain in a single scan. They also show how a new sparse sampling scheme enables acquisition of these biomarkers in just 14 min – significantly shorter than clinical multi-contrast MRI protocols that can take up to an hour.
“Our main motivation was to develop an ‘omni’ imaging technology that fully harnesses the rich biological information embedded in magnetic resonance signals, enabling us to unravel the structural, physiological and molecular fingerprints of brain function and diseases,” says Liang.
In vivo studies
MRI is widely used within brain tumour diagnosis to evaluate tumour location, size and extent, and blood–brain barrier disruption. However, standard MRI scans do not directly reveal the underlying pathophysiological changes and tumour heterogeneity. MRx, on the other hand, can acquire a wide range of biomarkers that provide valuable information on processes such as neuronal loss, energy metabolism, axonal damage, hypoxia, demyelination and many more.
To test the technique, Liang and colleagues performed MRx imaging on patients with clinically diagnosed brain tumours, using machine learning to combine the measured biomarkers into a single variable defining the tissue state at each pixel. This MRx “tissue state index” could differentiate eight distinct tissue states: grey matter; white matter; cerebrospinal fluid; oedema (fluid build-up); meningioma; low and high-grade oligodendroglioma; and glioblastoma. Standard multiparametric MRI failed to separate these states.
This ability to accurately characterize tissue states could enable a range of essential clinical tasks, such as grading low- versus high-grade brain tumours, for example, or separating glioblastoma from oedema during radiation therapy planning.
MRx could also prove invaluable for lesion characterization in multiple sclerosis (MS), a critical process for stratifying patients, planning treatment and predicting disease progression. The researchers demonstrated that MRx of patients with MS could differentiate active and chronic MS lesions without requiring contrast agents (as in current practice), attributed to the technique’s ability to visualize biomarkers specific to individual pathophysiological processes.
Such MRx biomarkers also helped to predict lesion progression, by capturing key pathophysiological features that cannot be revealed by conventional MRI, a feature that could enable early interventions and improve patient outcome.
Beyond cancer and MS, many other brain diseases could also benefit from MRx, including stroke, epilepsy and Alzheimer’s disease, for example. “MRx is expected to open up new opportunities for brain mapping and for precision healthcare of brain diseases, including neurological and neurodegenerative disorders,” says Liang.
For the proton-based studies reported in this latest study, MRx was performed without needing any modifications to the MRI scanner hardware. Instead, the method is implemented using a new pulse sequence for data acquisition plus custom software for data processing. Liang notes that extending MRx to include multiple nuclei – such as sodium, phosphorus, and deuterium – will require specialized multinuclear RF coil hardware.
“Our current efforts are focused on further improving the robustness and reliability of MRx under practical clinical imaging conditions, to facilitate both scientific studies and clinical translation,” he tells Physics World, noting that MRx has already been licensed (through Siemens) to imaging centres worldwide for evaluation of its clinical potential. “We are also expanding the technology to map additional molecular species and, ultimately, to enable multinuclear multiplexed imaging beyond protons.”
In the ongoing quest to improve cancer treatments, the radiation oncology community is looking to add to its armoury of radiation-based treatments. In particular, radiopharmaceutical therapy (RPT) – also known as molecular radiotherapy (MRT) – and the emerging sub-field of theranostics are set to play an expanded role as radiation medicine shifts towards a more integrated, multidisciplinary approach.
RPT is an evolving modality that uses a tumour-targeting molecule attached to a therapeutic radioisotope to deliver radiation directly to tumour cells. Theranostics takes this approach a step further, pairing the therapeutic radioisotope with a diagnostic analogue to image the disease before therapy and predict how the radioactive drug will be taken up by a specific patient.
“Interest in theranostics has really exploded since the clinical approvals of two radioactive drugs that are being used right now to treat patients,” explained Jeff Kapatoes, vice-president of regulatory, physics and product at Mirion Medical, at the recent QA & Dosimetry Symposium (QADS) hosted by Sun Nuclear.
The two approved drugs – Lutathera and Pluvicto – are approved for treating neuroendocrine tumours and certain prostate cancers, respectively, currently for later-stage disease but with multiple clinical trials ongoing to expand their remit to early-stage disease. “There are also active trials that treat other disease sites, such as lymphoma, breast and lung,” Kapatoes noted. Alongside, some 70 companies are developing their own therapeutic radiopharmaceuticals, with nine candidates now in phase-three trials and closing in on approval.
Emerging technologies Jeff Kapatoes of Mirion Medical introduced the session on theranostics at the QA & Dosimetry Symposium. (Courtesy: Sun Nuclear)
But despite its vast potential, theranostics is still in the early stages of widespread clinical adoption. While external-beam radiotherapy benefits from established treatment and quality assurance methodologies, this is simply not the case for theranostics. And as demand continues to grow, it’s vital that the full theranostic workflow is standardized – from radioisotope production through to final delivery to the patient.
Mirion Medical can support this integration of theranostics into radiation oncology, offering a broad portfolio of products designed for the entire theranostics lifecycle. The transition will also rely heavily on the contribution of medical physicists, who are uniquely positioned to implement theranostics programmes within their institutions.
Theranostics today
Speaking at the QADS event, John Sunderland from the University of Iowa explained the current situation. “The reality is, in external-beam radiotherapy, there are methods to ensure that the beam reaches the right place and the energy deposited is what you think. In RPT, you don’t control where the dose goes, biology and biochemistry do.”
He described a typical theranostic prostate cancer treatment, which begins with a PET/CT scan to visualize how a diagnostic radioisotope binds to the patient’s prostate cancer cells. Candidate patients are then injected with a therapeutic radioisotope comprising the same cancer-targeting molecule labelled with the beta emitter lutetium-177 (177Lu), which delivers highly localized radiation dose to the tumours. Importantly, this drug can also be imaged, using SPECT/CT to track its delivery.
Serial imaging enables treatment to be tailored to a patient’s response. Sunderland discussed one patient who had almost complete response after three treatments with Pluvicto (which is delivered in up to six cycles of 200 mCi). “There’s no reason to keep giving radiation dose to this patient, which might result in adverse events, we may as well stop,” he explained.
More typically, a patient will exhibit stable disease or a modest response – likely because not enough dose was delivered to the tumour. Simply increasing the amount of injected activity, however, risks increasing the dose to non-target organs such as kidneys or bone marrow. “Instead, we’re trying to move to dosimetry-modulated RPT where you modulate the amount of injected activity based upon the dosimetry in that first cycle,” Sunderland explained. “Then you can optimize the efficacy while maintaining critical organ toxicity levels to below where they might have adverse effects.”
Such dosimetry modulation requires three things: accurate measurement of the injected activity using a radionuclide calibrator; quantitative SPECT mapping of the absorbed radiation dose; and uniform software tools. But challenges remain, due to a lack of standardization at all three stages.
“Even expert physicists making the same dosimetry measurements with the same image data could vary by 20 to 30%, just because of the methodology they choose,” said Sunderland. “We have to standardize. We’re not where the external-beam people are, we’re all doing it differently because it’s so new.”
Challenges to address John Sunderland detailed the workflow for dosimetry-modulated radiopharmaceutical therapy. (Courtesy: Sun Nuclear)
The PDIB project
The Precision Dosimetry Imaging Biomarker (PDIB) project hopes to remedy this situation via three parallel projects: establishing a network of secondary standards calibration laboratories (SSCLs); standardization of SPECT/CT scanner calibration procedures; and standardization of dosimetry calculation workflows. “Only if we can do that are we actually going to be able to define our radiation dose-effect curves, as the external-beam field has been doing for years,” said Sunderland.
The first project aims to enable accurate measurement of the injected dose. To achieve this, four SSCLs – at BC Cancer, the University of Iowa, the University of Alabama Birmingham and the Belgian Nuclear Research Centre – will work with the national metrology labs NIST and NPL to support clinical trials worldwide. Using high-purity germanium detectors, the labs will perform absolute activity measurements of the six most commonly used radionuclides (177Lu, 131I, 225Ac, 111In, 203Pb and 212Pb). These samples can then be used by radiopharmacies and imaging/therapy sites to adjust their own dose calibrators to the SSCL measurements, targeting an overall activity uncertainty of less than 3%.
The second project, designed to harmonize quantitative calibration of SPECT/CT for therapeutic radionuclides, involves 12 imaging sites across the US, Europe and Australia. “There’s no standard way to calibrate right now and there’s no way to validate the calibration,” said Sunderland. The plan is to calibrate seven common quantitative SPECT/CT scanner models, using three different phantoms and the six radionuclides, using SSCL-supplied samples to ensure accurate activities.
The final project addresses the dosimetry calculations. Led by five international experts (two in North America, two in Europe and one in Australia), the project will examine 177Lu dosimetry for kidneys, bone marrow and tumours using 20 curated 177Lu-DOTATOC datasets. The teams will use five cases to develop standard operating procedures, then test these procedures on the other 15 cases, using five different dosimetry software packages, to investigate inter-user dosimetry variability.
“Radiopharmaceutical therapy is a big deal,” Sunderland emphasized. “The market for nuclear medicine is growing exponentially; it’s going to be double that of external-beam radiotherapy by 2030. And there are not nearly enough nuclear medicine physicists to do this work.”
In the US, RPT is a shared domain between radiation oncology and nuclear medicine, with active discussion around which department should be handling radiation for therapeutic versus purely diagnostic purposes. In Europe, meanwhile, theranostics generally sits solely within the remit of nuclear medicine.
“We need to recruit the external-beam physicists into the fold,” said Sunderland. “From a dosimetry and physics standpoint, there’s a lot of overlap here and a lot of expertise.”
Supporting the theranostics workflow
This blurring of traditional boundaries between nuclear medicine and radiation oncology creates both opportunities and complexities. With a comprehensive portfolio of products that span both domains, Mirion Medical aims to ease this convergence of disciplines and support the physicists navigating this transition.
Designed to standardize and streamline the full theranostics workflow, ec² Software enables radioisotope manufacturers, radiopharmacies and clinical facilities to provide traceability and support precision, safety and regulatory adherence.
“Products from ec² Software enhance precision through accurate dose tracking and documentation across the radiopharmaceutical lifecycle, improve safety by reducing manual steps, and support regulatory compliance with auditable records,” Kapatoes explained. “Overall, ec² Software helps health systems move from fragmented processes to consistent, scalable operations.”
Meanwhile, Mirion’s broader Radiopharma offering supports the physical and operational infrastructure required for safe and accurate delivery of theranostic procedures. This includes dose calibrators, SPECT calibration phantoms and shielding systems from Capintec, all of which will be key enablers for the introduction of dosimetry-modulated RPT.
“While ec² provides the workflow, traceability and compliance layer, Mirion’s hardware and monitoring solutions address the measurement, protection and safety environment in which those workflows operate,” said Kapatoes. “Together, they create an integrated approach, linking what’s happening operationally with what’s happening physically. This alignment helps health systems standardize processes, reduce variability and maintain compliance as programmes scale.”
A first-in-human study from researchers at the Mayo Clinic has shown how proton therapy could provide a new treatment option for patients with hard-to-treat ventricular tachycardia (VT), a life-threatening heart rhythm disorder. In the small group of patients examined in this early feasibility study, the treatment led to a 79% reduction in VT episodes.
VT is a type of abnormal heartbeat in which faulty electrical signals in the ventricles cause the heart to beat too quickly, meaning that it can’t pump enough blood around the body. Treatments include antiarrhythmic drugs or the use of catheter ablation to destroy the areas of myocardium (cardiac muscle) responsible for the abnormal signals. Sufferers can also be fitted with an implantable cardioverter-defibrillator (ICD) that automatically delivers a shock to reset the heart’s rhythm during a VT attack.
Some patients, however, don’t respond to conventional therapies, including antiarrhythmic medications and catheter ablations, and ICD shocks can significantly impact quality-of-life. For these cases, cardiac radioablation – which uses external-beam radiotherapy to target the problematic myocardium – is under investigation as an alternative, catheter-free treatment for VT.
Previous clinical studies of cardiac radioablation have employed photon-based irradiation, which can expose surrounding cardiac tissue to low-to-moderate radiation doses. Beams of protons, on the other hand, deposit almost all dose at a defined depth (the Bragg peak) and could enable more precise targeting with reduced irradiation of nearby healthy tissue.
“The main motivation for investigating cardiac radioablation is to improve upon the limitations and suboptimal outcomes of catheter ablation of VT in some patients,” explains lead investigator Konstantinos Siontis. “The motivation specific to protons is the potential dosimetric advantage, allowing more precise myocardial targeting while minimizing radiation to surrounding cardiac and extracardiac structures compared with photons.”
In this new study, reported in Heart Rhythm, Siontis and colleagues used proton-based cardiac radioablation to treat seven patients with advanced cardiomyopathy (disease of the heart muscle) and recurrent VT despite drug treatment and previous catheter ablations.
First-in-human investigation
To define the target myocardium for radioablation, the team integrated data from multiple imaging modalities (primarily MRI, plus CT) with information from electrocardiogram (ECG) and electrophysiology mapping originating from the patient’s prior invasive ablation procedures. The CT images were then used to contour the target and organs-at-risk (OARs) and for treatment planning.
The researchers designed treatment plans to deliver a single 30 Gy fraction of expiration-gated intensity-modulated proton therapy to the cardiac internal target volume (ITV, the target myocardium expanded to include cardiac motion) while sparing surrounding OARs. They point out that, due to safety uncertainties in thisfirst-in-human study, they took a generally conservative approach to target definition. In all patients, at least 90% of the ITV received 100% of the prescription dose, while a median of 96.2% of the ITV received at least 95%. Importantly, only 4.3% of non-target myocardium received a dose of 20 Gy or above.
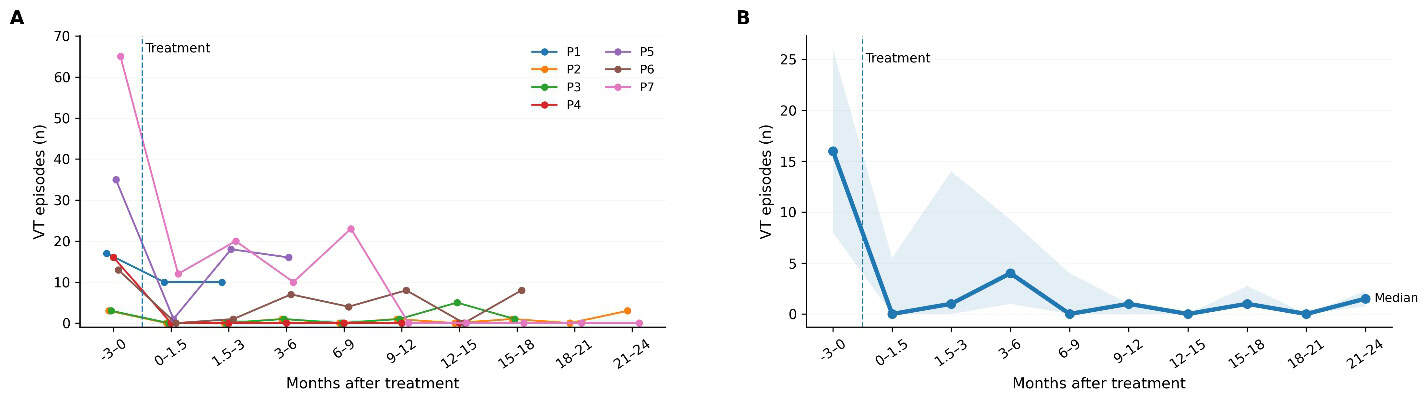
VT control A: VT episodes before and after treatment until each patient’s end of follow-up. B: the median number of VT events per patient in each time interval. (Courtesy: K C Siontis et al. Heart Rhythm 10.1016/j.hrthm.2026.04.021)
After treatment, the investigators performed follow-up evaluations for up to two years (median 514 days). Most patients experienced recurrent VT during this time, although less frequently than before the radioablation. Across all patients, the rate of VT events declined from 7.24 per patient-month in the three months before treatment to 1.52 per patient-month afterwards – corresponding to a 79% reduction in VT event rate. None of the group experienced serious treatment-related side effects and key heart function measures remained largely stable.
All patients in this study had advanced structural heart disease with severely reduced ventricular function and recurrent VT, putting them at high risk of both arrhythmic and heart failure-related mortality. In line with this profile, two patients required heart transplantation (at 66 and 514 days after treatment) and three died (at 155, 502 and 529 days), due to progressive heart failure.
“This early feasibility study demonstrates that proton cardiac radioablation for refractory VT can be safely planned and delivered with encouraging reductions in arrhythmic burden and no clear treatment-related toxicity,” the researchers conclude. “These findings support the feasibility of proton-based cardiac radioablation and justify further investigation,” they write.
Siontis notes that alongside the emergence of cardiac radioablation techniques, catheter ablation tools are also constantly improving. “Radioablation is unlikely to replace catheter ablation broadly, but it could become an important complementary or salvage option for patients with refractory VT who are poor candidates for invasive procedures,” he tells Physics World.
The team is now planning a larger prospective trial to better define the safety, efficacy and optimal targeting. “We are also investigating improved radiation delivery techniques, such as optimizing treatment planning around cardiac motion,” says Siontis. “In parallel, we continue to investigate photon radioablation in a pivotal randomized trial (RADIATE-VT), while we also offer proton therapy as a compassionate use option for patients in need in our clinical practice.”
Medical physics – the application of physics principles and techniques to medicine – plays a pivotal role within modern healthcare, with advances in the field serving to improve diagnostic accuracy, treatment precision and patient safety. But despite its immense potential to enhance patient care, medical physics in the UK faces various funding, regulatory and approval challenges that may prevent it from fulfilling this promise.
Taking a closer look at these obstacles, the Institute of Physics (IOP) has published a new community perspective report entitled Medical Physics in the UK: Opportunities and Challenges. The report examines the barriers to translation and commercialization of medical physics research, and proposes the next steps towards creating a more supportive environment for medical physics in the UK.
The report was instigated by the IOP Medical Physics Group and presents the conclusions of a series of discussions, held over two months, examining the challenges that medical physicists encounter in their daily work. The report also highlights the outcomes of an intensive two-day workshop examining the translation of quantum technologies into clinical applications.
The challenges and the opportunities
The UK has a strong legacy of leading medical physics research. To benchmark its contributions, the report authors analysed the top 5% most highly cited papers published in international medical physics journals from 2014 to 2023, revealing that the UK is fourth in the world for its research output in medical physics.
The UK also boasts a large, diverse medical technology industry and has the sixth largest medical device market globally. Notably, its research output involves a high proportion of non-academic co-authors – including corporate, government and clinical collaborators – suggesting a strong potential for translating physics research into the medical market.
The report identifies some of the challenges in realising this potential, including a stretched workforce and critical skills shortages, and outlines some of the more impactful obstacles – namely misaligned funding structures, a complex regulatory landscape, and lengthy approval processes for medical devices and clinical trials.
In the UK, medical physics research is funded by a combination of government agencies, charitable organizations, and independent trusts. The multidisciplinary nature of medical physics, however, risks promising projects falling into the gaps between funding categories, making it difficult for researchers to secure financial backing.
Navigating the regulatory landscape for medical physics developments is also a complex process, with different global markets having their own specific requirements. Challenges here include obtaining initial regulatory approval, adapting to evolving standards and managing multiple regulatory bodies simultaneously. And while new technologies are often sold into larger markets such as the USA and Germany, the UK’s medical device approval process lacks seamless integration with international regulatory bodies, creating barriers to such wider market adoption.
Finally, clinical trials and validation processes for medical physics innovations can often take several years. Securing funding for large-scale trials and collecting sufficient data to demonstrate long-term efficacy can also lead to delays in introducing new technologies to patients.
Overcoming these challenges will be key to fully exploiting the significant potential of medical physics to revolutionize healthcare in the UK. An initial step could be to bring together this diverse community – including researchers, medical practitioners, industry, NHS officials, government representatives and funders – to initiate a collaborative dialogue and brainstorm innovative strategies.
The report suggests three possible discussion points: how to better align funding mechanisms to support interdisciplinary research; how to shape an integrated regulatory framework with increased transparency; and how to strengthen collaboration between academia, healthcare and industry.
Such discussions should result in a comprehensive list of actionable recommendations. The report authors propose that the IOP establishes an impact project to explore the details of these recommendations and identify pragmatic, implementable solutions for their implementation.
For radiotherapy centres, daily quality assurance (QA) provides the final safety check before each day of patient treatments – ensuring that all linear accelerators (linacs) deliver radiation safely, accurately and as expected.
But as radiotherapy technologies evolve, the required QA procedures become increasingly complex, with verification tests often performed in isolation using multiple phantom set-ups. New treatment techniques – such as surface-guided radiotherapy (SGRT), which is more widely used now than ever – also introduce new QA requirements. And the ongoing adoption of adaptive radiotherapy, where measurement-based pre-treatment QA is not possible, increases the emphasis on machine QA, in which daily QA plays a key role.
What’s needed is a comprehensive QA approach that incorporates the dosimetry, imaging and positioning checks required for all radiotherapy modalities. Addressing this challenge, US manufacturer Sun Nuclear has launched Daily QA 4 Pro, a new device that simplifies daily machine QA by combining dosimetry and positioning verification via imaging into a single indexed, imageable platform.
“The main motivation for launching the Daily QA 4 Pro was to create a product that not only met the current needs of clinicians, but also future needs, based on our vision of the radiotherapy QA field,” explains Rajiv Lotey, technical product manager for the Daily QA 4 Pro.
The next-generation platform builds on the company’s Daily QA 3 beam quality analysis product, which was introduced more than a decade ago and is now standard in many radiotherapy departments. “The biggest difference between the Daily QA 4 Pro over the Daily QA 3 is the end-to-end QA functionality – representing the patient workflow – achieved by integrating a 3D high-resolution array, fiducials, an SGRT-compatible surface, an imageable architecture, and the ability to correlate all imaging and mechanical isocentres together onto one device,” says Lotey.
Enabling new modalities, expanding clinical applications
David Barbee, Director of Technology and Innovation in Radiation Oncology at NYU Langone Health, was one of the first to adopt this technology. Speaking at the recent QA & Dosimetry Symposium (QADS) hosted by Sun Nuclear, he described his early experiences of using the next-generation Daily QA 4 Pro.
“The first thing I wanted to do was evaluate surface-guided radiation therapy, because we don’t currently do this during daily QA,” Barbee explained.
To perform this test, the team defined a region-of-interest in the hospital’s VisionRT SGRT system that covered the entire surface and edges of the Daily QA 4 Pro and tested it over the full range of couch motion. The maximum translation range that it could detect was about ±4.5 cm in the lateral (side to side) and longitudinal (along the couch length) directions, and +13 to –17 cm vertically.
“For pitch and roll, we tested the 3°/3 mm limits and 90° couch rotations, and it observed them perfectly,” he added. “This is the first time we’ve ever run this test and compared our SGRT system to our image guidance system,” he noted. “This is very, very helpful.”
Quality and patient safety in radiotherapy Attendees at the QADS15 event shared best practice strategies and clinical insights with colleagues practicing worldwide. (Courtesy: Sun Nuclear)
For dosimetry, Barbee noted that many parameters are carried over from the Daily QA 3 – including the output profile constancy, the field size and shift, and the flatness and symmetry – but added that the Daily QA 4 Pro can measure at a much wider range, anywhere from 2 to 20 cm square fields. “There are also new metrics, such as the penumbra, beam shape constancy for FFF [flattening filter-free] fields, the beam centre and the dose-per-pulse,” he explained. “And there’s a new dose output correction factor for when you need to move this device to a different unit.”
Barbee and colleagues performed a range of dosimetry assessments using the Daily QA 4 Pro, measuring 30 sessions on six linacs using both jaw- and multi-leaf collimator (MLC)-defined field sizes. They found that the output factors were consistent down to about 7 mm, after which the MLC gave slightly higher output factors, while the largest beam profile differences were seen in flatness and symmetry for very small fields.
Integrating Winston–Lutz
The Daily QA 4 Pro incorporates active measurement Winston-Lutz tests – a standard procedure for evaluating isocentre accuracy – using the system’s onboard 3D detector array to directly measure the radiation isocentre. The NYU Langone team used the Daily QA 4 Pro to quantitatively assess the mechanical isocentres and their response to gantry, collimator and couch motion for six linacs, again using both jaw- and MLC-defined fields.
Barbee noted that the system runs the gantry and collimator checks automatically. “You can basically hit play on SunCHECK and then you don’t touch anything again until you get to the couch, which you have to move from the console,” he explained.
To test the accuracy of the results, Barbee compared them with two years’ worth of Machine Performance Check (MPC) and traditional Winston-Lutz measurements of all of the centre’s linacs. Daily QA 4 Pro measurements agreed well with previous isocentre results across all machines tested. “It’s a little bit early to say, but it looks commensurate, there are no concerns,” he noted.
A look inside the device
The Daily QA 4 Pro measures 30 x 50 x 6 cm, weighs 6.2 kg and sits on a 4.1 kg six degrees-of-freedom base. It incorporates four ion chambers that measure field sizes down to 5 x 5 cm, as well as 249 diodes spaced at high resolution in the x– and y-directions, the diagonals and along both sides. There are also eight 3 mm tungsten carbide BBs positioned off-axis, factory-calibrated to enable micron-level corrections.
The Daily QA 4 Pro.
Externally, the device incorporates scribed laser alignment marks with 2 mm tolerance on its sides and surfaces, plus a crosshair for collimator alignment. There are also field size markings for 5 x 5, 10 x 10 and 20 x 20 cm fields, as well as eight symmetric reliefs designed specifically for SGRT.
The Daily QA 4 software is designed to integrate into the SunCHECK environment and can be controlled using either SunCHECK Local via a standalone laptop or (starting in version 6.0) the SunCHECK Server.
The team also ran active imaging Winston-Lutz tests, which evaluate system geometry by analysing the position of a known target in images acquired using the linac’s imaging panels. The Daily QA 4 Pro device detects the image fiducials (tungsten carbide BBs) and compares their positions to expected values for each gantry angle. These tests allow users to assess factors such as device positioning, gantry angle accuracy and overall alignment.
“This is all summarized into a report showing the maximum error in any one of those parameters across all gantry angles,” explained Barbee. “It will tell you which gantry angle was the worst and what the value there was.”
Used together, the two Winston-Lutz methods combine direct radiation measurement with imaging-based verification to provide a more complete understanding of system health and to help identify, quantify and correct any errors.
Efficiency analysis
Barbee notes that while the Daily QA 4 Pro generates a comprehensive set of dosimetry and positioning verification data, at first glance, it looks like a lot more work. An efficiency analysis, however, proved the opposite – demonstrating significant gains in workflow efficiency.
Currently, Daily QA 3 and IGRT tasks take about 16 min to perform. “Daily QA 4 Pro cuts about five minutes off that time, because you’re not going in and out of the room and doing multiple setups,” he explained. “Adding Winston-Lutz currently doubles the time to over half an hour. But with Daily QA 4 Pro, you only add five minutes. And it’s a simple setup that your therapist can run as part of their morning QA.”
“The Daily QA 4 Pro integrates image-guided radiotherapy, SGRT, beam dosimetry and Winston-Lutz verification into a single device, enabling comprehensive daily QA in a single setup and session,” Barbee concluded. “This provides an independent, interpretable alternative to vendor black-box QA systems, with comparable isocentre and imager tests, and superior beam quality constancy tests. It really can consolidate a lot of phantoms that you might not need anymore.”
The discovery of X-rays and radioactivity in the late 19th century gave rise to a surge of interest from the scientific community, shortly followed by the realization of the adverse effects of ionizing radiations on health. By about 1910 the dangers were widely recognised and some basic protection measures were being adopted. It was not until 1934, however, that the first quantitative standards of radiological protection were published.
Of course, protection against the adverse effects of ionizing radiation is as important today as ever, particularly for those working within nuclear and defence-related industries, medicine and R&D, as well as hospital patients undergoing radiation-based procedures and members of the general public. As such, the last century has seen the development of a complex international regulatory system, with recommendations on occupational and public exposures to radiation – from organizations such as the International Commission on Radiological Protection (ICRP) and others – continually revised and updated.
A new book, Principles and Techniques of Radiological Protection, provides a comprehensive overview of the current regulatory context for radiological protection. The text also provides an overview of the scientific issues relating to radiological protection and the current state-of-the-art tools used to comply with the relevant legislation and guidance.
Targeted at postgraduate students and new entrants to the field, the textbook is designed to cover a wide range of topics that an early-career radiation protection professional might need, or want, to know about. It also serves as a day-to-day reference work for specialists such as radiation protection advisors (RPAs) to identify appropriate techniques to address radiological protection issues as they arise.
“I aimed to produce a book that I would have liked to have had available when I started work in radiological protection just over 50 years ago,” explains the book’s editor Michael Thorne. “As I come towards the end of my career in the field, I aimed to include information, tools and techniques that I would have liked to have had readily accessible in a single volume.”
History, theory and practical applications
Thorne begins the book with a brief history of radiological protection and how historical developments continue to influence the discipline today. The next chapters examine the physical aspects of radiological protection, including an overview of basic nuclear physics and the sources of radiation, radiation transport through and interactions with matter, and the instruments used to detect and monitor radiation. Later chapters cover the principles of internal dosimetry, phantoms and biokinetic models, and mathematical modelling of radionuclide transport.
Michael Thorne A chartered radiation protection professional with 50 years of experience, Thorne is editor-in-chief of the Journal of Radiological Protection and consultant at Mike Thorne and Associates Limited. (Courtesy: Michael Thorne)
“I have also given a detailed account of natural background radiation and modelling the transport of radionuclides in the environment; and I have included a chapter on the effects of radiation on the environment, with specific emphasis on non-human biota,” says Thorne. “Throughout, I have recruited co-authors with decades of relevant experience to capture their expertise in each of the specialized areas.”
The book also provides examples of how this information is employed practically within various fields, including the nuclear industry and industries handling naturally occurring radioactive materials. Several chapters and themes are of particular relevance to those working within medical physics.
“There are two chapters specifically on radiology and nuclear medicine, written by Colin Martin, who is well known internationally for his work in this area,” Thorne tells Physics World. “There are also specialized chapters on biokinetic modelling, the nature and use of both mathematical and physical phantoms in radiation dosimetry, and on the use and abuse of instruments for radiation monitoring.”
The book rounds off with a look at the some of the major and minor accidents that led to exposure of members of the public and workers using radioactive sources. The final chapter addresses emergency planning and response for such incidents, including suggested protective actions and the roles and responsibilities of various organizations.
“Throughout, the emphasis is on broad principles and widely applicable techniques,” says Thorne. “It is considered that an individual who gains a clear understanding of these principles and techniques will be readily able to apply that understanding to the diverse and changing set of challenges that arise.”
Individual copies of Principles and Techniques of Radiological Protection can be purchased at the IOP Publishing Bookstore.
Stanford Medicine has opened a new proton therapy facility – featuring an ultracompact treatment system that’s small enough to fit in a room the size of a conventional linear accelerator vault.
Proton therapy is an advanced cancer treatment that offers precise tumour targeting while minimizing dose to healthy tissues. The technique is particularly beneficial for treating tumours located near critical structures and for treating cancers in children. Currently, however, access to proton therapy is limited by its high costs and substantial space requirements.
The new treatment facility – opened earlier this week at Stanford Medicine Cancer Center in Palo Alto, CA – incorporates the S250-FIT proton therapy system from Mevion Medical Systems, the most compact cyclotron in the industry. But even with a much small accelerator, proton therapy delivery usually requires a bulky gantry that rotates around the patient to aim the proton beams at the optimal treatment angles. As such, most proton facilities need a whole new multi-storey building to be built just to fit everything in.
To eliminate this obstacle, the Stanford facility is using a positioning system from Leo Cancer Care to deliver protons via a novel approach known as upright radiotherapy. Here, the patient is treated in an upright position (rather than lying down) and rotated in front of a static treatment beam, removing the need for a gantry and slashing space requirements and installation costs.
Mafe to fit Installation of the compact cyclotron. (Courtesy: Stanford Medicine)
By combining these advanced technologies, the new equipment fits into a standard 1200 sq. ft linear accelerator vault (as used for standard X-ray-based radiotherapy) and was installed without having to construct a new building.
The advanced system also incorporates built-in CT scanning, enabling extremely precise targeting of tumours within patients with minimal collateral damage to the rest of the body.
“Developing this novel approach to proton therapy at Stanford Medicine, in collaboration with our industrial partners Mevion and Leo Cancer Care, gives us an important additional tool to treat our patients in a personalized, case-by-case way,” says Billy Loo, professor of radiation oncology and co-director of particle therapy at Stanford Medicine. “We are excited to pioneer this world’s first ultracompact and efficient technology that will benefit not only patients at Stanford but expand access to proton therapy worldwide and improve patient outcomes.”
“This milestone really marks the transition from concept and theory to clinical reality,” adds Leo Cancer Care’s CEO Stephen Towe. “Proton therapy installed inside a linac vault always felt like an impossible goal – our partnership with Stanford and Mevion has made that vision possible.”
Loo tells Physics World that patient treatments on the new proton therapy system are likely to start this summer. “As with any first-of-its-kind system in medicine, introducing this complex technology requires a rigorous process of testing and optimization to ensure it meets our high standards for patient safety and treatment quality,” he explains. “We are moving through these steps now.”
The Stanford Medicine team emphasize the particular advantages of proton therapy for children, not least that it can really decrease the radiation dose delivered to normal tissues. Minimizing irradiation of sensitive developing tissue can dramatically reduce the risk of long-term side effects. In addition, treating children while they are sitting up and actively engaged may be far less intimidating for them than having to lie down and have the treatment “happen to them”.
Official launch The proton therapy facility at Stanford Medicine Cancer Center was opened on 7 April with a ribbon-cutting ceremony. (Courtesy: Steve Fisch, Stanford Medicine)
The first proton treatments will likely be “cranial and head-and-neck sites, for both adults and selected paediatric patients, for which we already have established patient positioning solutions,” says Loo. In parallel, the radiation oncology team will develop the workflows and immobilization solutions for all other anatomic sites.
The team also plans to investigate new ways to advance the technology and explore the clinical advantages of delivering upright radiotherapy. For example, evidence suggests that for some diseases, such as lung cancer, upright treatment puts the targeted organ in a more favourable position to irradiate safely. Upright positioning also provides greater flexibility to deliver radiation from many different angles. The team will also study the impact of upright positioning on FLASH treatments, in which radiation is delivered at ultrahigh dose rates.
Looking ahead, nine other medical centres are installing this new ultracompact proton therapy system, ultimately making proton therapy increasingly accessible to patients around the world.
“The clinical data to support the use of protons is stronger than ever before,” says Towe. “The strength of this data, combined with the cost reductions delivered by Leo’s technology, has sparked a new wave of growth for protons globally.”
This episode of the Physics World Weekly podcast features Brian Pogue, who is professor of biomedical engineering at Dartmouth College in the US. He is also the co-founder of several start-up companies that are developing optics-based systems for medicine.
In conversation with Physics World’s Tami Freeman, Pogue explains that optical technologies underlie many of today’s routine medical procedures. The field of optics is also converging with the world of medical physics, and Pogue talks about exciting new techniques for guidance, dosimetry and in vivo verification of radiation therapy cancer treatments.
This interview was recorded in association with the journal Physics in Medicine & Biology, which celebrates its 70th anniversary this year.
This podcast is supported by One Physics, your trusted, local partner in medical physics and radiation safety.